PHOENIX — Dr. Diane Meier won a MacArthur Foundation “genius1” grant in 2008 for her pioneering work in palliative medicine, which seeks to optimize patients’ quality of life by preventing or reducing their suffering.
That journey, she said, started on the first morning of her internship — during which she assisted in an hour-long, fruitless effort to resuscitate an 89-year-old man with end-stage heart disease — and culminated in 1999 with her cofounding of the Center to Advance Palliative Care.
Meier is vice chair for public policy and professor of palliative medicine at the Icahn School of Medicine at Mount Sinai. When she spoke here on a recent day at the annual meeting of hospice and palliative care specialists, there wasn’t a single empty chair in the room.
You’ve been critical about our culture’s increasing focus on discussing and accepting death, and how that could affect the medical community.
I am not critical of the cultural openness to this element of the human experience. Rather, I think the job of health professionals is to help our patients and their families live as well and as fully as possible while they are alive.
We in medicine should not be in the business trying to sell people the idea that death is OK. Death is never going to be OK. And it feels a bit self-righteous to me — as if we are saying it’s a moral obligation for people to prepare for their own death. It makes me very uncomfortable, because that impulse is more about us than about the people we’re trying to serve.
The people we’re trying to serve have serious illnesses, and they’re trying to live as well as they can for as long as they can. This notion that somehow you’re braver or smarter or wiser if you confront your death and accept it and plan for it — this is not what most patients and families are seeking. It’s not what most people care about. And it actually can get in the way of people having a good life.
How so?
Because quite naturally, all living things try to avoid death, and are afraid of death. And by focusing on that inevitable event, you’re not living in the present. You’re letting your life be defined by the fear of death.
Can’t the awareness of death help you live more consciously in the present?
Yes. And as a physician, I have a much greater appreciation for the value of present moment, because I’ve taken care of so many people who had fewer moments than they wanted. But I don’t feel like it’s my job to impose that awareness or approach to life on my patients.
Are there any redeeming qualities in this movement?
I think there are societal advantages to it being permissible to talk about the fact of death and its inevitability. People who are facing death perhaps feel less marginalized or beyond the pale, literally, if it’s an acceptable mainstream conversation. And achieving the good death — where death is not full of pain or shortness of breath, or fear, or families falling apart — I think that’s a societal good. But I don’t think you get there by forcing people to face the fact of their mortality.
And it’s not our job as health professionals to be convincing people that it’s OK to die, and that death is natural and death is good. It flies in the face of millions of years of human evolution. It’s not OK to die. Very few people want to die, particularly if they have a quality of life that’s acceptable to them. Life is precious, and sweet, and my job as a physician is to help my patients get as much of that good quality life as they can.
Some of the people who helped start this movement, like Atul Gawande, probed death and dying in order to prompt a conversation about quality of life. He wrote about a diabetic man who was near death, but the medical staff was still micromanaging his diet. The quote was something like, ‘Let him have the damn cookie.’
That’s exactly my point. It’s about helping people live the kind of life that they want. Being in the moment with them.
For a patient, accepting death …
That’s somebody else’s agenda. When they talk to me about it, patients are mostly afraid of what might happen before they die. Will they be short of breath? In pain? And it’s amazing how reassured people are to know that for the great majority of people death is very peaceful. And in the unusual instances where there are symptoms like pain and shortness of breath or confusion or restlessness, we have very effective medicines for those things.
So do you think this societal focus on accepting death will continue to intensify?
There are generational cycles where death is in vogue. Think about Elisabeth Kubler Ross and her book “On Death and Dying,” which had a huge readership. And now we’ve got Paul Kalanithi and Atul Gawande and “Extremis.”2 It does cycle, this generational rediscovering the fact of death. And now it’s kind of hip, because it’s Silicon Valley. It’s Ideo [the design firm that launched an initiative called “Redesigning Death”]. Cool people are writing about it. Fine. Good. But is this going to change how human beings from time immemorial have thought about and feared their own death? I don’t think so.
And, as you’ve pointed out, we’re more than a little obsessed with immortality too.
The medical profession has quite explicitly become about the defeat of death. Go to the NIH websites: The mission is to eliminate cancer. Eliminate dementia. Eliminate heart disease. As if their true goal is bodily immortality. Now let’s think about that for a minute, and what it’d mean for our society. And yet there’s not even a whiff of irony about this.
Certainly we want to eliminate childhood deaths, premature death. But do we really want to be pouring the entire Treasury into eliminating death among old people? It’s an unquestioned assumption that it’s good. That’s the air we’re breathing. And I think the question is not one of forcing people to look in the mirror and say, “You’re going to die.” The right question is, “What’s a good life for you? How can I as a clinician wrestle the resources and capacities of the health care system into something that’ll serve what matters most to you?”
Site: The Economist
A STROLL from Todoroki station, at the kink of a path lined with cherry trees, lies a small wooden temple. A baby Buddha sits on the sill. The residents of the Tokyo suburb ask the infant for pin pin korori. It is a wish for two things. The first is a long, spry life. The second is a quick and painless death.
Just part of this wish is likely to be granted. The paradox of modern medicine is that people are living longer, and yet doing so with more disease. Death is rarely either quick or painless. Often it is traumatic. As the end nears, people tend to have goals that matter more than eking out every last second. But too few are asked what matters most to them. In the rich world most people die in a hospital or nursing home, often after pointless, aggressive treatment. Many die alone, confused and in pain.
The distress is largely unnecessary. Fortunately medicine is beginning to take a more thoughtful approach to people with terminal illness. Reformers are overhauling how end-of-life care is delivered and improving communication between doctors and patients. The changes mean that patients will experience less pain and suffering. And they will have more control over their lives, right up until the end.
Many aspects of death changed during the 20th century. One was when it happens. The average lifespan increased by more over the past four generations than over the previous 8,000. In 1900 global life expectancy at birth was about 32 years, little more than at the dawn of agriculture. It is now 71.8 years. In large part that is a result of lower infant and child mortality; a century ago about a third of children died before their fifth birthday. But it is also because adults live longer. Today a 50-year-old Englishman can expect to live for another 33 years, 13 more than in 1900.
The chance of an adult dying was once largely unrelated to age; infections were indiscriminate. Michel de Montaigne, a French essayist who died in 1592, wrote that death in old age was “rare, singular and extraordinary”. Now, says Katherine Sleeman of King’s College London, death mostly comes by stealth. She estimates that in Britain only a fifth of deaths are sudden, for example in a car crash. Another fifth follow a swift decline, as with some cancer patients, who stay fairly active until their final few weeks. But three-fifths come after years of relapse and recovery. They involve a “slow, progressive deterioration of function”, Dr Sleeman says.
People in rich countries can spend eight to ten years seriously ill at the end of life. Chronic illness is rising in poorer countries, too. In 2015 it accounted for more than three-quarters of premature mortality in China, according to the Global Burden of Disease, a survey. In 1990 the share was just a half. The World Health Organisation (WHO) predicts that rates of cancer and heart disease in Sub-Saharan Africa will more than double by 2030.
A side-effect of progress, however, has been what Atul Gawande, a surgeon and author, calls “the experiment of making mortality a medical experience”. A century ago most deaths were at home. Now, according to a survey of 45 rich countries by the WHO, fewer than a third are. Death also used to be egalitarian, says Haider Warraich of Duke University Medical Centre and the author of “Modern Death”. Income did not much affect when or where people died. Today poor people in rich countries are more likely than their better-off compatriots to die in hospital.
No dying fall
Many deaths are preceded by a surge of treatment, often pointless. A survey of doctors in Japan found that 90% expected that patients with tubes inserted into their windpipes would never recover. Yet a fifth of patients who die in the country’s hospitals have been intubated. An eighth of Americans with terminal cancer receive chemotherapy in their final fortnight, despite it offering no benefit at such a late stage. Nearly a third of elderly Americans undergo surgery during their final year; 8% do so in their last week.
The way health care is funded encourages over-treatment. Hospitals are paid for doing things to people, not for preventing pain. And not only patients, but those who love them, suffer. Many people who may need intubation or artificial ventilation are not in a condition to indicate consent. An American study found that in about half of cases involving decisions about the withdrawal of treatment there is conflict between family and doctors. A third of relatives of patients in intensive-care units (ICUs) report symptoms of post-traumatic stress disorder.
Many people will want to “rage, rage against the dying of the light”, as the poet Dylan Thomas put it. Others will have particular events they want to attend: a grandchild’s graduation, say. But the medical crescendo often occurs by default, not as a result of personal choice based on a clearly understood prognosis.
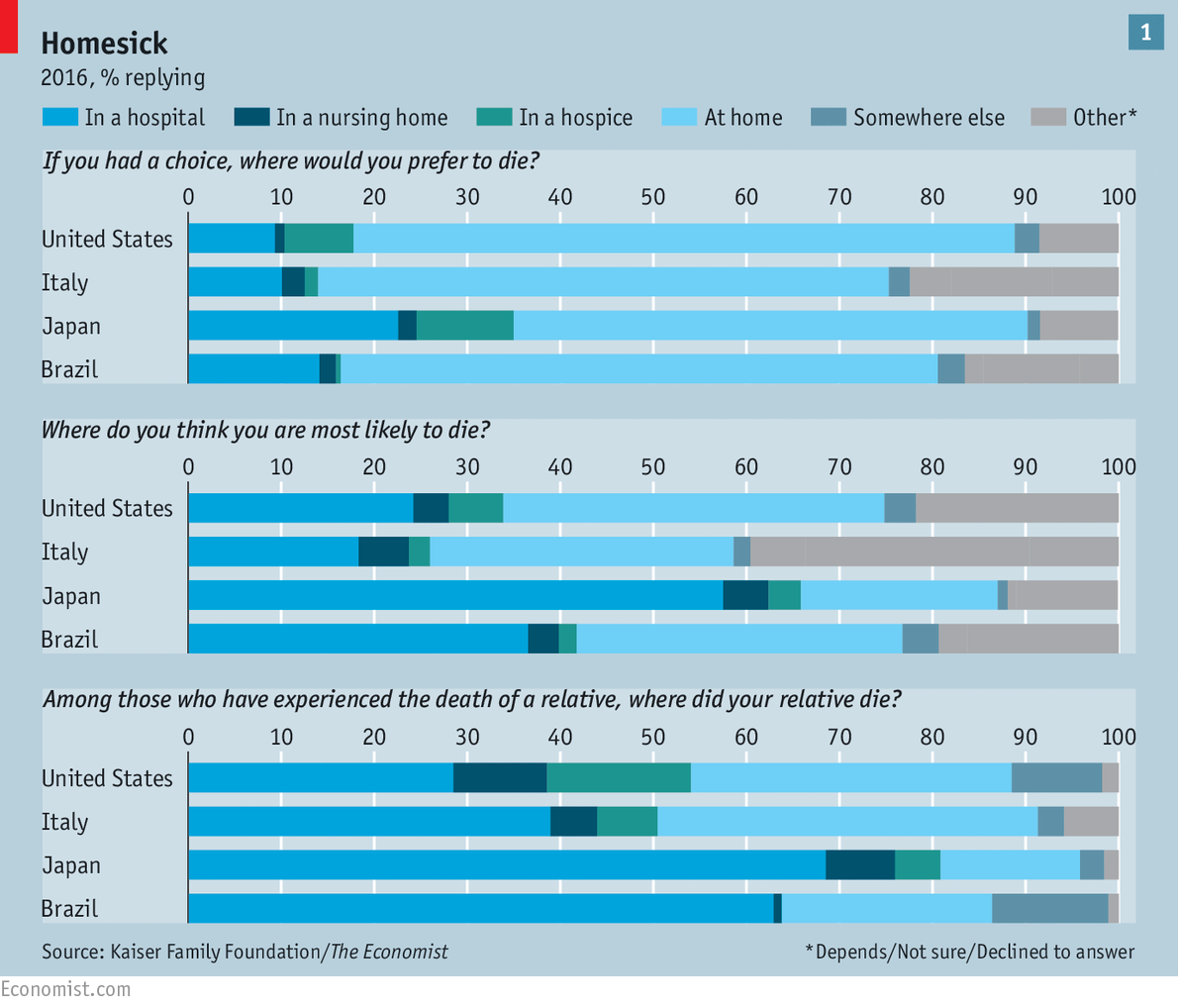
The huge gap between what people want from end-of-life care and what they are likely to get is visible in a survey conducted by The Economist in partnership with the Kaiser Family Foundation, an American health-care think-tank. Representative samples of people in four large countries with differing demographics, religious traditions and levels of development (America, Brazil, Italy and Japan) were asked a set of questions about dying and end-of-life care. Most had lost close friends or family in the previous five years.
In all four countries the majority of people said they hoped to die at home (see chart 1). But fewer said they expected to do so—and even fewer said that their deceased loved ones had. Apart from in Brazil, only small shares said that extending life as long as possible was more important than dying without pain, discomfort and stress (see article). Other research suggests that wish, too, is increasingly unlikely to be granted. One study found that between 1998 and 2010 the shares of Americans experiencing confusion, depression and pain in their final year all increased.
What healthy people think they will want when they are mortally ill may well change when that moment comes. “Life becomes mighty precious when there is not a lot left,” says Diane Meier, a geriatrician at Mount Sinai Hospital in New York. It is common, for example, to hate the idea of a feeding tube but grudgingly accept one when the alternative is death.
Words I never thought to speak
Yet the gap between what people hope for and what they get cannot be explained away so easily. Dying people’s wishes are often unknown or ignored. Among those involved in making decisions about a loved one’s end-of-life care, more than a third in Italy, Japan and Brazil said they did not know what their friend or family member wanted. Either they never asked, or only thought to do so too late. A Japanese woman who cared for her mother, an Alzheimer’s patient, says she regrets that “once the door closed there was no way of knowing what she wanted.”
And sometimes, even when relatives know a loved one’s wishes, they cannot make sure they are granted. Between 12% and 24% of those who had lost someone close to them said that the patient’s wishes had not been carried out. Between 25% and 38% said that friends or family had experienced needless pain. Across the whole survey most people rated the quality of end-of-life care as “fair” or “poor”.
End-of-life care can resemble a “conspiracy of silence”, says Robert Fine of Baylor Scott & White Health, a Texan health-care provider. In our survey majorities in all four countries said that death is a subject which is generally avoided. An obvious reason is that death is feared. “In every calm and reasonable person there is a hidden second person scared witless about death,” says the narrator of a Philip Roth novel. One school of psychology—“terror management theory”—holds that fear of death is the source of everything distinctively human, from phobias to religion.
But death was once what Philippe Ariès, a French historian, called a “public ceremony”, where friends and family gathered. Now, changing family structures mean the elderly and dying are more isolated from younger people, who are therefore less likely to witness death up close, or to find a suitable moment to talk about its approach. Just 10% of Europeans aged over 80 live with their families; half live alone. By 2020, 40% of Americans are expected to die alone in nursing homes.
In Japan, where survey respondents were most likely to say that not being a financial burden was a primary consideration, daughters are abandoning their traditional caring role. That has given rise to institutions such as the House of Hope, a hospice in east Tokyo that looks after people who are too poor for hospital care and too alone to die at home. A decade ago Hisako Yanagida, 88, lost her husband, with whom she had sung in a traditional Japanese troupe. Now her sight is going but she can still make out the faded pictures of the two of them on her wall. She tries not to think about death: “There is no point.”
But the chief responsibility for the failures of end-of-life care lies with medicine. The relationship between doctors and seriously ill patients is one of “mutual suspicion”, says Naoki Ikegami of St Luke’s International University, in Tokyo. A decade ago it was common for Japanese doctors to withhold cancer diagnoses. Today they are more honest, but still insensitive. One Japanese woman recalls her oncologist saying that if her chemotherapy made her bald, it would not be a big deal.
And doctors commonly overestimate how long the terminally ill will live, making it more likely that they will duck frank conversations, or recommend drastic treatments that have little chance of success. One international review of prognoses of patients who die within two months suggests that seriously ill people live on average little more than half as long as their doctors suggested they would. Another study found that, for patients who died within four weeks of receiving a prognosis, doctors had predicted the date to within a week in just a quarter of cases. Mostly, they had erred on the side of optimism.
Doctors often neglect palliative care, which involves giving opioids for pain, treating breathlessness and counselling patients. (The name comes from the Latin palliare, as in “to cloak” pain.) A typical question is “What is important to you now?” It does not seek to cure. As a result, “it is seen as what you do when you give up on a patient,” sighs Dr Ikegami. It receives just 0.2% of the funding for cancer research in Britain and 1% in America.
Breaking the taboo
What studies there have been show the cost of this neglect. Since 2009 several randomised controlled trials have looked at what happens when patients with advanced cancer are given palliative care alongside standard treatment, such as chemotherapy. In each, the group receiving palliative care had lower rates of depression; and in all but one study, patients in that group were less likely to report pain.
Remarkably, in three trials the patients receiving palliative care lived longer, even though the quantity of conventional treatment they opted to receive was lower. (The other two trials showed no difference.) In one study their median survival was a year, compared with nine months for the group receiving only ordinary treatment. A review in 2016 of cases where palliative care was used instead of standard treatment found that even when it was the only care given, it did not seem to shorten life.
The reason for the results is unclear, and the research has mostly been on cancer patients. Those receiving palliative care spend less time in hospital, so may contract fewer infections. But some researchers think that the explanation is psychological: that through counselling they reduce depression, which is linked to earlier death. “A conversation can be more powerful than technology,” says Dr Sleeman.
At St Luke’s hospital in Tokyo, Yuki Asano supports the argument. Ever the executive, the 76-year-old slides his business card across the tray of his bed. The former boss of a brewery company (and 7th dan in kendo, a Japanese martial art) is riddled with cancer. He stopped chemotherapy last year. The care at one of Japan’s few dedicated palliative centres has helped him feel ready for death. “I achieved everything I wanted in life,” he says. “Now I am waiting for the awards ceremony.”
But few of the 56m or so people who die each year receive good end-of-life care. A report published in 2015 by the Economist Intelligence Unit, our sister company, assessed the “quality of death” in 80 countries. Only Austria and America, the EIU found, had the capacity to ensure that at least half the patients for whom palliative care was suitable received it.
Many countries promise public access to palliative care but do not pay for it. Spain has passed two laws to ensure palliative care is available but in reality, just a quarter of patients can get it. Though the hospice movement, dedicated to providing high-quality care to dying patients, started in Britain in the 1960s, only about a fifth of the country’s hospitals provide access to palliative care every day of the week.
The way health-care providers are funded often sidelines palliative care. In Japan hospital doctors receive no payment from insurers for talking to patients about end-of-life options. In America hospitals suck up a big share of spending, even though the seriously ill are often better treated elsewhere. Nine in ten emergency visits are because of escalations in symptoms, such as breathlessness; most of these patients could be treated better, faster and more cheaply at home. Medicare, the public-health scheme for the elderly, does not generally cover spells in nursing homes.
Slowly, however, countries are reforming. In 2014 the WHO recommended integrating palliative care with health systems. Some developing countries, including Ecuador, Mongolia and Sri Lanka, are beginning to do so. In America some insurers are realising that what would be better for patients would be better for them, too. In 2015 Medicare announced that it would pay for conversations about end-of-life care between doctors and patients.
“Talking almost always helps and yet we don’t talk,” says Susan Block of Harvard Medical School. To improve end-of-life care, she says, “every doctor needs to be an expert in communicating.” American oncologists, for example, need to have an average of 35 conversations per month about end-of-life care. In a study of patients with congestive heart failure, doctors rarely followed up after a patient expressed a fear of death. Nearly three-quarters of nephrologists were never taught how to tell patients they are dying. A common cause of burnout among doctors is an inability to talk with patients about death.
To fill this gap Ariadne Labs, a research group founded by Dr Gawande, has launched the “Serious Illness Conversation Guide”. It is a straightforward checklist of the topics doctors should be sure to talk about with their terminally ill patients. They should start by asking what patients understand about their conditions, check how much each wants to know, offer an honest prognosis, and ask about their goals and the trade-offs each is willing to make.
Early results from a trial of the guide at the Dana-Farber Cancer Institute in Boston suggest it led to doctors having more and earlier conversations. Patients reported less anxiety. Tension between doctors and families was eased. The scheme is being expanded; in February Baylor Scott & White became the first big provider to use it for all its staff. England’s National Health Service is trying it out in Clatterbridge, near Liverpool. Japan is retraining its oncologists in how to talk about death.
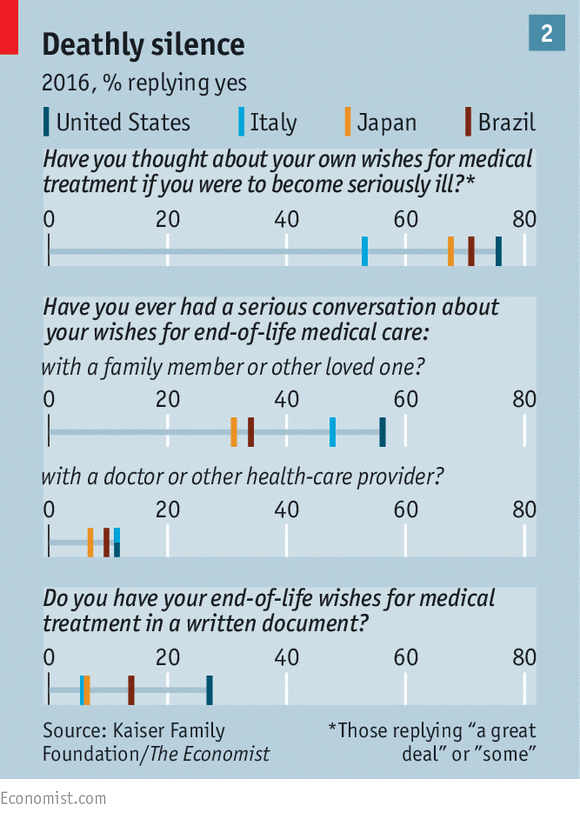
In America advance directives and living wills, documents that spell out the treatment people want if they become incapacitated, have become more popular over the past few decades. In our survey 51% of Americans over 65 had written down their end-of-life wishes. Yet such documents cannot cover all the possibilities that may arise as the end nears. Doctors worry that patients may have changed their minds. In one study just 43% of people who had written living wills wanted the same treatment course two years later.
Living wills are rare outside America (see chart 2). But there is a broader cultural shift. More than 4,400 “death cafés”, where people eat cake and talk about mortality, have sprung up. They discuss books such as “When Breath Becomes Air”, by the late Paul Kalanithi, a neurosurgeon, and the documentary “Extremis”, which is set in an intensive-care unit and offers a more honest account of hospital care than in popular TV shows. In Japan “ending notebooks” are now available, to record messages and instructions for relatives.
Here at the end of all things
In 2010 Ellen Goodman, an American author, founded the Conversation Project, which started with people gathering to share stories of the “good deaths” and “bad deaths” experienced by their loved ones. It publishes guides like those from Ariadne Labs, but for use by people without medical training. Laurie Kay from Boston, who is 70, recently told her husband and daughter that what mattered to her was dignity. She wants to look good: her nails should be painted. Her views may change, she says, but “having opened the conversation now we can reopen it later.”
Experiences of death are being shared online. Dying Matters is a popular forum. In 2013 Scott Simon, a journalist, tweeted from his mother’s bedside as she died (“Heart rate dropping. Heart dropping”, read one tweet). Kate Granger, an English geriatrician who died of cancer last year, planned to tweet during her final days using the tag #deathbedlive. She did not quite manage it, but a tweet she prepared was sent posthumously: “TY all for being part of my life. Pls look after my amazing hubby @PointonChris (Ps - Don’t let him spend all his money on a Range Rover) xx”.
Bringing death “within the pale of conversation” is needed to overhaul end-of-life care, argues Dr Warraich. Yet the “death positive” movement is not an excuse for medicine to remain stuck in its ways. Death will remain terrifying for many people. Unless the way health care is organised changes, most people will continue to suffer unnecessarily at the end. Correction (April 30th): A previous version of this piece said that Laurie Kay is in her 80s. She is in fact only 70. Apologies.
 Courtesy Diane Meier
Courtesy Diane Meier